Wrist instability and wrist ligament injuries
The wrist is a complex joint. In fact it is really two neighbouring joints, the radio-carpal and the mid-carpal joints (see figure).
There are two rows of wrist bones, the “proximal” and “distal” carpal rows. These are nestled together at the mid-carpal joint and the two of them rest on the radius and TFCC, overlying the ulna.
The bones of each of the carpal rows are bound together with short inelastic ligaments. And the two rows are bound to each other and to the radius and ulna by longer, more pliable ligaments (see figure).
What is stability? Stability is the state of normal alignment of a joint through a normal range of loading and motion. When a joint intermittently becomes malaligned, then it suffers from instability. The patient may feel the joint give way with a clunk, or if the instability is less obvious, then it may just cause pain after activities.
If a patient has a fall and tears a wrist ligament, this may result in the ligament no longer functioning normally. If the bones no longer maintain their normal alignment, then instability is the result.
Some patients have excessively loose ligaments, and as a result of this, abnormal motion can occur.
In both those cases, hand therapy may help strengthen and activate secondary stabilisers which can maintain the alignment of the bones. An example would be improving a specific muscle’s tone and activity to help prevent the abnormal motion. This depends on the ligaments affected. Sometimes surgery is required to reconstruct the insufficient ligament.
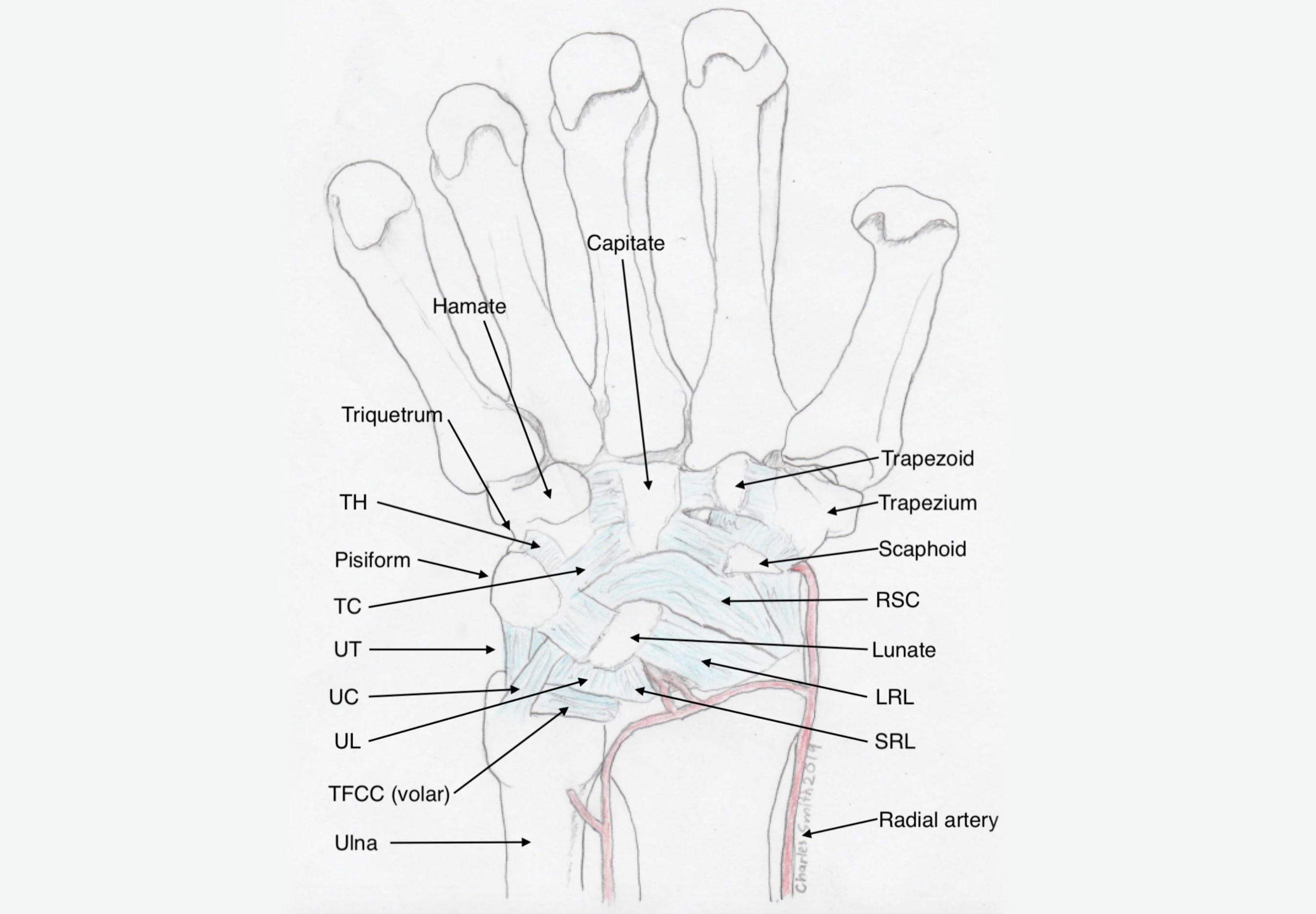
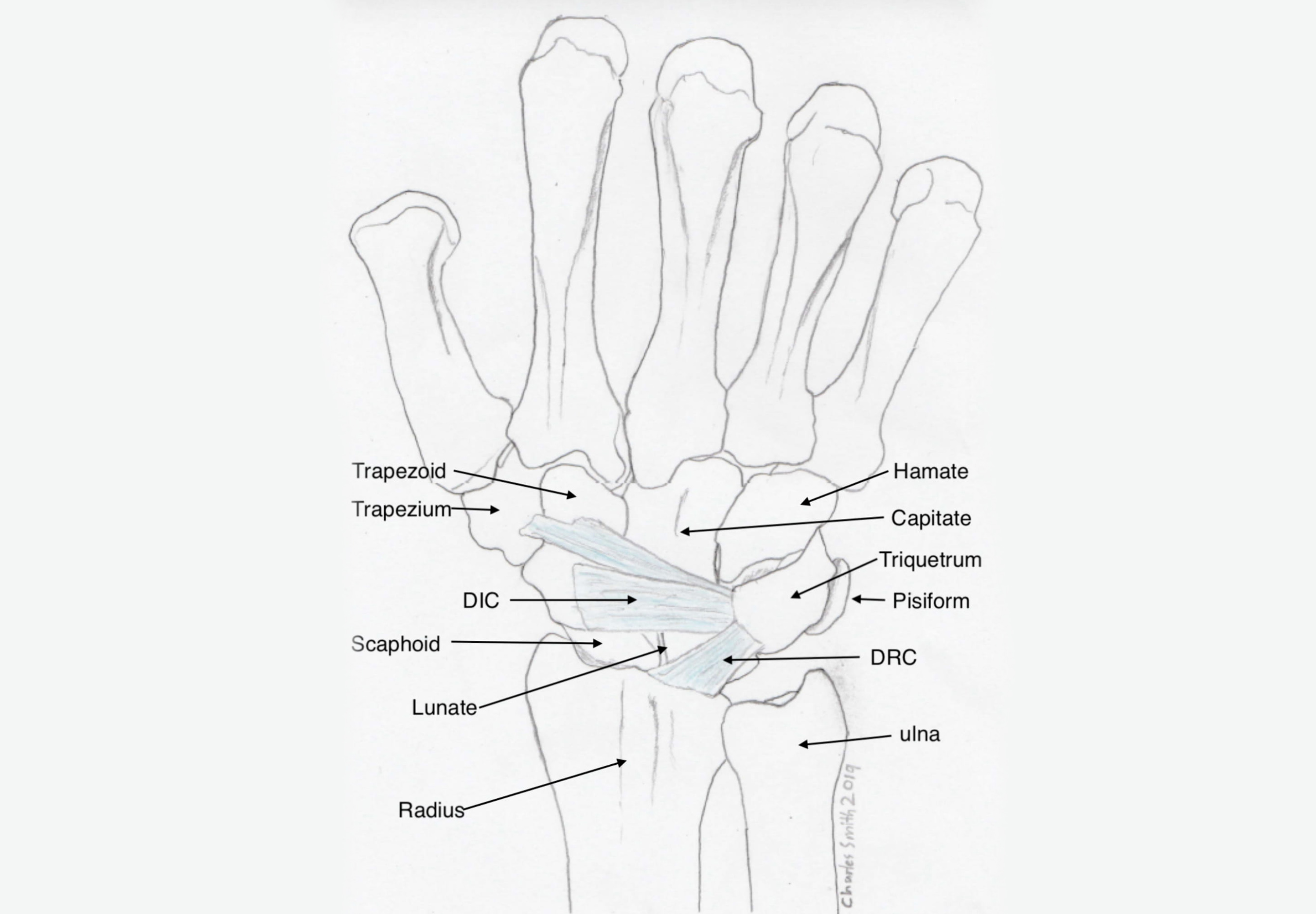
Top: volar wrist ligaments, Bottom: dorsal wrist ligaments


Scapholunate ligament deficiency
The scapholunate ligament is the c-shaped ligament that binds the scaphoid to the lunate (see diagram).
The palmar and middle parts of the ligament are the weakest. The thick dorsal (fingernail side) band is the most important. Additional fibres from inside the wrist capsule reinforce the dorsal band (DCSS)
The ligament is usually damaged with a fall onto the hand. Pain and swelling will follow and x-rays will usually be normal. This is a difficult diagnosis to make initially, unless the ligament is so badly injured that a gap between the bones is visible on the x-rays. Anyone with pain and swelling and normal x-rays after a wrist injury may have an injury to this ligament. Unlike with scaphoid fractures, MRI scans are not always diagnostic, in fact there is no perfect way to image this structure reliably, at least not yet. Accurate diagnosis requires a careful arthroscopic evaluation, but this is not really advisable for everybody with a sore wrist.
When the scapholunate ligament is deficient, abnormal motion develops between the scaphoid and the lunate, and with loading, the scaphoid can slip in relation to the radius. This can cause ongoing pain, clunking and can fairly rapidly lead to wrist arthritis or SLAC wrist (scapholunate advanced collapse).
When the scapholunate ligament is deficient, abnormal motion develops between the scaphoid and the lunate, and with loading, the scaphoid can slip in relation to the radius. This can cause ongoing pain, clunking and can fairly rapidly lead to wrist arthritis or SLAC wrist (scapholunate advanced collapse).
Until recently, I was so disappointed with the results of ligament reconstruction, that I did not recommended it for my patients. Apart from being unreliable in restoring stability, these reconstructions seemed to have great potential to make the wrist more stiff than it was before. This stiffness related to the need for pins crossing the joint for 12 weeks, to protect the reconstruction. The wrist remained in cast until the wires were removed.
My view on this changed after visiting Paco del Pinal in Spain, who showed me the arthroscopic ligament reconstruction of Corella, a young hand surgeon also from Spain. This reconstruction does not require the use of K-wires, and does minimal additional damage to the wrist. Although we are still refining the indications for the use of this surgery, it definitely results in marked improvement for many patients with this problem. The surgery is very technical, and still in the “too hard basket” for many, but it is definitely a step in the right direction, in my opinion (see photos).
For patients where there is still some dorsal ligament remaining, the arthroscopic suture technique of Christophe Mathoulin seems to be an effective option also. Again, wire fixation is not required, and so no bridges are burnt. This is a reasonable option when a scapholunate ligament tear is incidentally discovered during arthroscopy for a distal radius fracture. In this scenario, the use of K-wires and immobilisation would certainly compromise the result following the fracture surgery, where early mobilisation should be a priority.
Midcarpal instability
Midcarpal instability refers to abnormal motion occurring between the two rows of carpal bones. Often this is associated with “generalised ligamentous laxity” rather than with a specific ligamentous lesion. As such, it is usually more effectively treated with hand therapy, where specific strengthening exercises allow the patient to regain control over the joint alignment.

