Dupuytren’s Disease
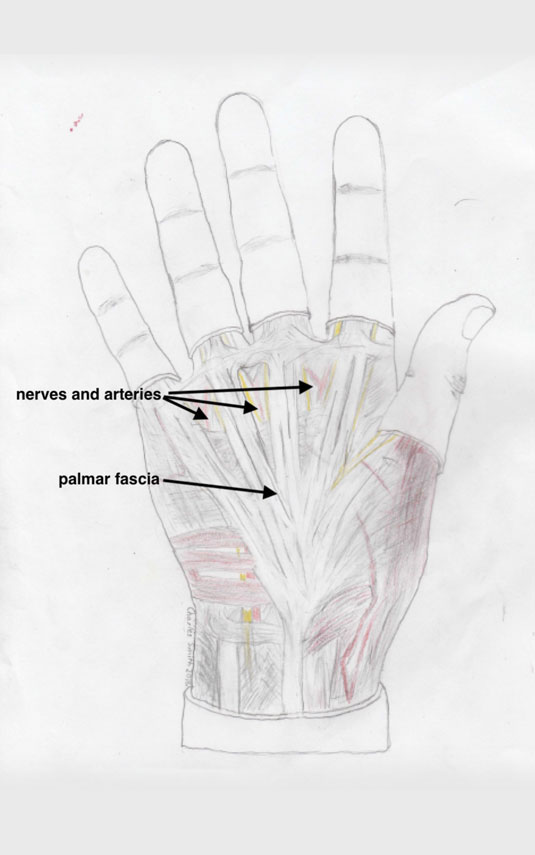
Dupuytren’s disease (DD) is a condition primarily affecting the palmar fascia. The palmar fascia is a fibrous scaffolding which normally connects the skin of the palm to the underlying skeleton. This helps support the skin of the palm when gripping, and stops the skin shearing off under loads. This effect can be seen if you wiggle the skin of the palm and compare it with the skin over the back of the hand.
In genetically predisposed people, the cells of the palmar fascia undergo a change and become contractile. Initially, lumps appear, which may be painful or itchy. Subsequently, parts of the palmar fascia shorten into “cords”, and thus typically flex one or more digits. When the process is well advanced, there may be tightening of all the structures in the digit – skin, nerves, arteries, tendons, small muscles, and joint ligaments.
In the initial phases of the disease, when there are pain and lumpiness, any attempt to break up the bands with surgery or other methods should be avoided. Such treatment during this early stage carries the risk of causing a marked flare-up of the disease.
After the shortening phase has begun, patients may feel that the position of the digit is causing problems. Some patients poke themselves in the eye with their little finger when washing their faces or shaving. Others just find the digit is in the way.
(PHASES OF DISEASE IMAGE – TBA)
When assessing the affected hand, surgeons will assess where the disease is located and which joints are affected. It is important to note previous treatment attempts, and if there seems to be a strong genetic predisposition or “diathesis”.
Traditional thresholds for doing something are if the hand can’t go, palm, down flat on a table or if the PIP joint is stuck in more than 30 degrees of flexion (see photos).

Effective treatment options are:
- percutaneous needle aponeurotomy (PNA) – where under local anaesthetic in the office, bands in the palm are broken up with a hypodermic needle.
- collagenase injections – where a small quantity of the recombinant bacterial enzyme “collagenase” is injected into the cord. The patient returns to the office a few days later to have the softened cord manipulated by the surgeon.
- surgery – of varying levels of complexity.
PNA and collagenase injections are more convenient for the patient when appropriate. The results of these two treatments are the same, in terms of recurrence after 2 years (roughly 50%).
My preference is towards PNA, which is simple and inexpensive. The cost to the patient for the collagenase is more than $1200 (Aus), not including any payment to the doctor. Collagenase also carries the side effect of alot of temporary swelling in many patients, and not infrequently causes some skin tears in the palm. Avoiding wounds in the palm is one of the reasons to avoid surgery! Collagenase also carries the rare risk of flexor tendon rupture, which is a pretty serious complication.
Surgery for Dupuytren’s disease remains a very effective option. It is my preferred method of treatment when the cord extends into the finger and is causing more than 30 degrees of flexion of the PIP joint (the second from the fingertip).
Where there is a severe contracture, sometimes my advice is to correct the problem with staged surgery, starting in the palm. This gives the nerves, arteries, and muscles time to adapt.
What to expect after PNA/Surgery
PNA-
After PNA a light dressing is applied to the hand for 24 hours. There is no real wound, so patients can get their hands wet after the dressing comes off. Some mild tenderness in the area is normal, but most patients are back to normal activities after a week. Hand therapy is not usually required.
Surgery-
After surgery, there are sutures, and often some open areas, left deliberately, which must be kept clean and dry. The sutures are removed at 14 days, and the open areas are usually healed at this stage. The hand can then get wet.
Hand therapy is often required to help maintain the improvement in movement achieved with surgery. This is usually for about 4 weeks.
When surgery has been used to correct more severe contractures, more prolonged hand therapy is sometimes required.

