Fractures
Introduction
There are 14 phalangeal and 5 metacarpal bones in the hand, with 19 associated joints. It is possible to injure each bone in many different locations, leading to an enormous range of fracture types.
The hand skeleton is all about movement, a movement that we tend to take for granted.
Limiting hand movement, for any reason, is a big mistake! Hand surgeons have a saying “that for every hand bone we see which doesn’t heal, we see 100 stiff hands”.
Stiffness
In medical language, the term “stiffness” means lack of normal motion in a joint. It does not refer to the feeling of muscle ache we might feel the day after a big run!
The setting of a hand fracture is a perfect situation to create finger stiffness. The bleeding and swelling from the broken bone are like glue waiting to set. The associated pain cause the fingers to rest in a protected position, which is more likely to result in stiff joints.
Casts versus splints
Casts in the hand are very likely to increase the chance of stiffness. In my practice, they are very rarely used.
Unlike casts, splints can be easily removed by the patient, so that they can move their joints. Their purpose in the setting of fractures is to promote healthy resting joint position and to provide some protection of the injured hand.
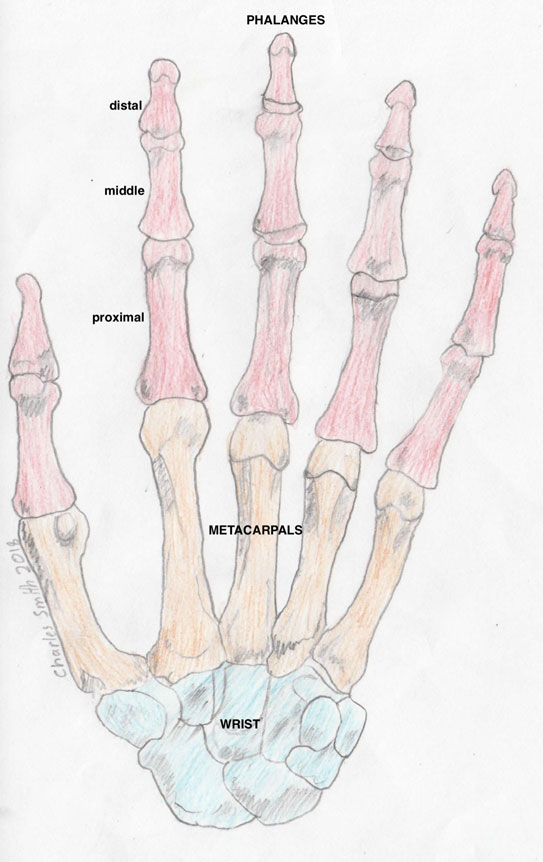
Hand and wrist bones

Top: fracture fixation with plate and screws, Bottom: fracture fixation with screws only
Movement
Whilst it might seem counter-intuitive to a non-doctor, it is important to move the hand as soon as possible after a fracture.
Before we begin a movement, we must decide that the fracture is “stable” or deduce that the fracture is “unstable”, in which case we should make it stable with a surgical procedure.
Stability
If on the x-rays there is angulation or displacement (shift) through the fracture, then it is usually unstable. If the fracture line appears like a crack, then it is probably stable.
The goal of surgery in displaced fractures is to perfectly realign the bone ends and hold them in such a way as to allow movement. The fixation should be minimally irritating to the soft-tissues and low profile.
Rehabilitation
Movement begins when the fracture is stable. A splint is used when the hand is resting, to prevent joint stiffness in unhealthy positions. Once the hand is freely mobile, the splint is probably not required.
Return to normal activities is usually delayed until bone healing has occurred on the x-rays. Typically this is about 8 weeks following the injury.
Competitive athletes may assume a degree of risk and return to normal prior to 8 weeks, depending on the type of fracture and how it has been fixed. Contact sports persons may return to play as early as 2 weeks, following robust fixation of metacarpal fractures.

